- Transplant
- Medical
- Cosmetics
- Transplant Packages
- Medical Packages
- Cosmetic Packages
- Hospitals
- Hotels
- Blog
- About Us
- Agents
 English
English
English
English
English

The most common spinal deformities are:
• Scoliosis – This is the most common deformity of the spine, which is accompanied by its flexion and rotation.
• Kyphosis excess (hyperkyphosis) – spinal deformity in the form of an arc facing back. Kyphosis is most often formed in the thoracic spine. The cause of excess kyphosis may be Sherman Mau’s disease.
• Sherman Mau disease–This is a disease in which several wedge-shaped vertebrae form in the middle thoracic spine, and as a result, a so-called “youthful hump” is formed. Sherman Mau’s disease can be accompanied by multiple hernias.
• Excessive lordosis– bending of the spine in the form of an arc facing forward. Excessive lordosis most often occurs in the cervical or lumbar spine. It can also be a manifestation of spondylolisthesis.
• Spondylolisthesis–Straction of the vertebra. A spinal disease associated with the inability of the upper vertebra to be held in a stable position relative to the lower one. Spondylolisthesis is of two types: degenerative, which occurs as a result of the destruction of the intervertebral disc or joints, and lytic – as a result of a fatigue fracture of the inter-articular part of the vertebral arch.
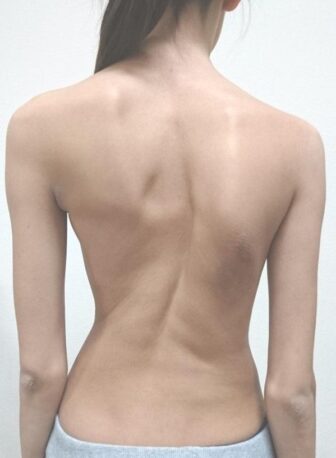
The main symptom of a spinal deformity is an abnormal curvature of the back. In kyphosis, the upper back is abnormally rounded. In scoliosis, the spine is curved to either side, and an exaggerated inward curve of the low back is known as lumbar lordosis.
In addition to this, a spinal deformity can cause severe pain in the back, which especially increases with movement. The cause of this pain is compression of the spinal cord or its nerves.
Sometimes spinal deformity can cause compression of inner organs and disorders of their functions. In severe cases, it can affect your lungs, heart, nerves, and other tissues.
Some symptoms occur only with certain types of spinal deformities. For example, in scoliosis, the ribs may be more prominent on one side due to the rotation of the spine from its usual position.
Kyphosis deformity of the spine and immobility of the thoracic region can cause forward positioning of the head compared to the rest of the body.
In lordosis, a large gap occurs between the lumbar region of the spine and the floor when you lie on your back. It results in chronic pain and tightness in the back.
Your spine is made up of three segments. When viewed from the side, these segments form three natural curves. The ‘c-shaped’ curves of the neck (cervical spine) and lower back (lumbar spine) are called lordosis. The ‘reverse c-shaped’ curve of the chest (thoracic spine) is called kyphosis. These curves are important to our balance and they help us to stand upright. If anyone of the curves becomes too large or too small, it becomes difficult to stand up straight and our posture appears abnormal. Abnormal curving of the spine is also referred to as spinal deformity. There are two main types of spinal deformity:
• kyphosis – a forward bend of the spine
• Scoliosis – a sideways curve of the spine.
A spinal deformity can be associated with a hunchback, swayback or rib humps.
There are many reasons why you can get a spinal deformity. Most commonly it is due to wear and tear of the spine with age, or a deformity which was present when you were a teenager and has persisted into adulthood.
Spinal deformity surgery aims to correct and control your spinal curving and improve your spinal balance. This is usually done by using metal screws, rods, plates and sometimes cages (known as metalwork) to permanently fuse certain segments of your spine. The metalwork initially acts as a scaffold while your bone gradually fuses (bony union) over a period of nine to 12 months.
There are three types of spinal deformity surgery:
• posterior instrumented fusion to correct the curving of the spine by fusing the vertebrae (bones forming the spine) from the back of the spine
• anterior instrumented fusion to correct the curving of the spine by fusing the vertebrae from the front of the spine
• complex deformity correction where parts of the vertebrae may be carefully ‘broken’ (this is called osteotomy of the spine) to achieve a better spinal balance.
Your surgeon will have already discussed with you why they think this is the best procedure to help with your condition.
There are many reasons for doing deformity surgery but the most common ones are related to:
• Progressive spinal imbalance causing pain and discomfort
• Risk of progression of spinal curving to a size where internal organs may be affected
• Failure of previous spinal metalwork: please refer to your doctor for any questions
• Fracture, infection or tumor of your spine:
please refer to your doctor for any questions.
Based on your symptoms and the results of MRI and/or CT scans and x-rays, your surgeon will decide exactly which level of vertebrae need fusing.
Deformity surgery is used for therapeutic purposes. The main aim of the operation is to correct, control and achieve spinal balance by fusing your spine. It is not a procedure to improve chronic pain.
It is difficult to predict how much your symptoms will improve after the operation. The real benefit is the improvement in the quality of life.
In general, the risks of spinal deformity surgery relate to the anesthetic (it will be done when you are asleep under general anesthetic) and the procedure itself.
For more information about having an anesthetic please see our leaflet, Having an anesthetic. If you do not have a copy, please ask us for one. If you are having sedation, you will be able to discuss this with the anesthetist before surgery and he/she will identify the best method for you.
Other pain-relieving therapies can help ease back pain and sciatica, such as pain-relieving medicines, spinal injections, and TENS (transcutaneous electrical nerve stimulation) machine. Exercise, acupuncture, yoga/Pilates and relaxation therapy may also help ease back pain.
Please refer to the following leaflet which will provide information on how to prepare for your operation:
During your pre-assessment, you should tell your nurse about any health conditions you have, such as diabetes, or bleeding disorders, and about any medicines that you may be taking, including blood-thinning and over-the-
counter medicines. You may be asked to stop taking certain medicines for several days before the procedure.
If you are a woman of child-bearing age, you must tell your nurse if you could be pregnant. If unsure, you will be asked to have a pregnancy test. This is because x- rays are usually used during the procedure. They are safe for adults but may harm your developing baby. If you are pregnant, your doctor will talk about alternatives to the procedure.
We want to involve you in decisions about your care and treatment. If you decide to go ahead, you will be asked to sign a consent form. This states that you agree to have the treatment and you understand what it involves.
You should receive the leaflet, Helping you decide: our consent policy, which gives you more information. If you do not, please ask a member of staff caring for you for a copy.
On your day of admission, you will be seen by a doctor who will mark the site of the surgery and ask you to sign the consent form. The anesthetist may also review your fitness for surgery and finalize the planned anesthetic regime. You will then be taken to the operating theatre.
If you are having an anterior instrumented fusion, you will lie on your side. If you are having a posterior instrumented fusion, you will lie on your stomach on a special mattress.
Your surgeon will make an incision (cut) on your skin after the level of vertebrae that need fusing has been confirmed.
During posterior fusion, the metal screws are inserted into your vertebrae and are held together by rods. If a cage is used, this is inserted into space where your disc is found (intervertebral disc space).
During anterior fusion, a portion of your rib will be cut and your lungs will be moved aside. The discs at the side where your spine is curved will be removed and filled with a bone graft (transplanted bone tissue). Then screws are placed into the vertebrae and connected with a rod or plate.
After your procedure, your doctor may choose to insert a suction drain (a thin tube attached to a measuring bottle that helps to remove fluids collected after an operation) before closing the skin with absorbable sutures (stitches). A local anesthetic may sometimes be applied to the operated area to relieve pain. You will also have pressure dressings.
The operation normally takes between four and six hours depending on the level of vertebrae that needs fusing and the complexity of your spinal problem. You will need to stay in the hospital for seven to 10 days after this procedure.
You should expect to have some tenderness at the operation site which will last up to 72 hours. You may have more back pain initially but this will settle down with time.
The local anesthetic should keep you relatively pain- free for a while, but it is best to take things easy for the first 24 hours.
You will also be given painkillers when staying in hospital but please let the doctors and nurses know if you are still in pain.
Following the operation, you will be taken to the Intensive Care Unit (ICU). This is where you are monitored for the initial post-operative period. You will be transferred to an orthopedic ward when your pain is under control and there are no concerns about your recovery.
You will need to lie on your back for up to eight hours after your operation. This will allow pressure to be applied to the operated site to reduce the amount of bleeding.
The morning after the operation, you can sit up at any angle. You will be seen by a physiotherapist who will help you walk depending on your pain and confidence. You will only be allowed to move around by yourself when the physiotherapist feels it is safe for you to do so. You will also be shown some simple exercises that you can do when you are at home. If you have any concerns about your walking, numbness or controlling your bladder/bowel, please tell a member of staff.
The pressure dressing and drain, if you have one, will be removed before you go home. You will be given antibiotics and blood-thinning injections after your operation to minimize the risk of infection and blood clots. You will need an x-ray of your spine before you leave the hospital.
You will need to arrange for a responsible adult to collect you from a hospital, preferably in a car. Travel on public transport is not recommended.
You must continue to take painkillers as advised after your surgery. Your pharmacist and nurse will discuss with you the management of your painkillers before you go home.
The dressing needs to be kept on until your wound is reviewed by your GP’s practice nurse seven to 10 days after the procedure. Once this has happened, you can have a bath or shower as normal without the dressing. If you have any concerns about the wound, please contact your GP or the ward staff immediately.
Bending and lifting should be avoided for six months. You can generally get back to light work after eight to 12 weeks (check with your employer) and can do heavier work and sports after 12 months. You are usually safe to drive within six to eight weeks provided that you can do an emergency stop (please refer to your insurance provider).
When you leave hospital you may be referred for physiotherapy either at IranMedTour or at your local hospital. Physiotherapists will teach you specific exercises to help tone and control the muscles that stabilize the lower back.
If you have been referred for physiotherapy, you should expect to have an appointment four to six weeks after your surgery date. If you are due to have physiotherapy at your local hospital and have not heard from them by this time regarding your appointment, please contact your GP.
If your pain does not settle within four to six weeks, you can either be reviewed in your scheduled outpatient appointment or you can contact your GP for advice and pain management.
Please contact your GP if you experience any of the following:
• excruciating pain unlike your normal symptoms
• increasing redness, swelling or oozing around the operation site
• fever (temperature higher than 38.5°C)
• sudden weakness or numbness which is not resolving
• sudden loss of bowel or bladder control
• severe headache which is not improved with painkillers.
Yes, six to eight weeks after your surgery. We will send you an appointment letter but if you have not heard from us within four weeks after leaving the hospital, please contact us. At this appointment, you will have an x-ray of your spine, and you will be seen by a physiotherapist or a doctor, depending on your pre-operative symptoms.

