- Transplant
- Medical
- Cosmetics
- Transplant Packages
- Medical Packages
- Cosmetic Packages
- Hospitals
- Hotels
- Blog
- About Us
- Agents
 English
English
English
English
English
EEP Prosthesis (Endo – Exo – Leg implantation) is one of the services of Iranmedtour, which is provided by the best surgeons, along with accommodation, translator, companion nurse, and city tour at an affordable price in Iran.
Amputation of a limb, unfortunately, can lead to severe constrictions for those affected in everyday life. Thus, one major aim of prosthetic rehabilitation is to regain non-restrictive mobility as much as possible.
Your desire to actively take part in every area of life is one of our strongest ambitions. On this page, we want to introduce a ground-breaking procedure that has proven its value for rehabilitation after limb loss for more than ten years by now. The exceptional feature of this technique is the absence of a socket and thus its lack of problems related to the conventional method. It can help you considerably to regain your mobility.
This website wants to inform you about the Endo – Exo – Prosthesis and gives an outline of the possibilities for rehabilitation after the above- or below-knee amputation using osseointegrated (bone-anchored) and percutaneous (skin penetrating) implants.
Our team accompanies you from the first counsel, the operation (implantation of the prosthesis), and throughout the post-op period with rehabilitation including physiotherapy and pain management as well as follow-ups. We also maintain a close relationship with you after you regained your mobility to make sure you always have a partner to turn to if there are any problems.
Independent mobility and quality of life will have a new meaning for you.
In 1990 first implantations of osseointegrated, percutaneous (skin perforating) femoral prostheses were performed by R. BRANEMARK, who provided a bilateral above knee amputee with an intramedullary (inside the bone) force carrier to which the conventional exo-prostheses could be attached. This idea derived from findings made with tooth implants. BRANEMARK’s father had invented tooth implants, which are also directly attached to the bone to allow the fixation of an artificial tooth. This system has found worldwide appreciation and is nowadays performed very often.
In 1999 the first so-called Endo-Exo-Femurprosthesis, which had been developed by Dr. Hans GRUNDEI, was implanted in a young motorbike rider after he suffered from a traumatic above-knee amputation of the left leg.
At the ISPO World Congress 2010 in Leipzig, Germany BRANEMARK reported by now more than 200 patients who had received his osseointegrated system mainly after traumatic amputations at above-knee, above- and below-elbow as well as thumb level.
The group in Lübeck, Germany around Dr. ASCHOFF can look at more than 100 patients that have been operated on in Lübeck itself and other patients in different places in Germany and other European countries as well as Australia.
Lübeck is the place with the highest amount of EEP – patients, there are also more than ten patients that have been provided with Endo-Exo-Tibia-Implants after a below-knee amputation. The third group in England has less clinical experience but intensely works on the problem of chronic soft tissue infection at the site of skin penetration of the implant, which has not been completely solved by now. A successful emulation of the biologic model of deer antlers is pursued. However, a closed system with a smooth transition from vital skin and soft tissue layers to the metal surface of the implant has not been achieved by now. The group in Lübeck around Dr. ASCHOFF, therefore, counts on a potential epithelialization (tissue growing) of the channel between the outer skin and the distal (away from the body) end of the bone. This thought is empirically driven due to the findings that in the case of complete skin growth inside of this channel an ascending infection is only theoretically possible between bone and implant. This is not obligatory but constitutes an absolute exception.

Integral Leg Prosthesis System surgical procedure performed in IRAN. 3D Animation created for iranmedtour.com
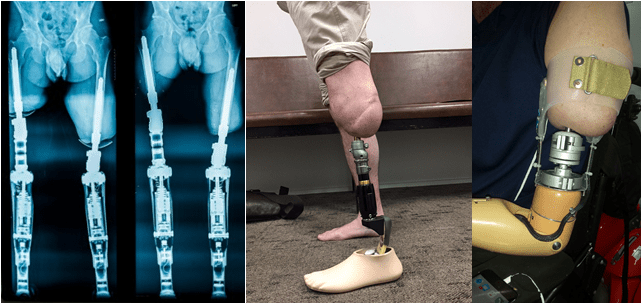
The EEP is made up of several modules. They can be subdivided into an inner module and an external module. The inner module, the so-called stem, is directly implanted into the remaining bone (i.e. femur, tibia, or humerus).
One special feature of the implant is the pa-tented Spongiosa-Metal® II surface. This surface allows the bone to grow through its three-dimensional grid structure (osseointegration), which secures a stable fixation of the prosthesis.
The dual cone adapter connects the internal and external modules. Fixed internally, it leads out of the stump and perforates the skin at the so-called stoma region creating a direct pathway from the inside to the outside components.
The silicone cover is used to protect the de-scribed stoma. The sleeve and the rotation disc serve as mechanical connections for the following knee connecting adapter, the artificial knee joint, and/ or the lower artificial limb prosthetic system. All the artificial joint components can be quickly and easily linked to the internal prosthesis using the knee connection adapter.
People with above or below knee amputations seek to return to a mobile lifestyle. Conventional rehabilitation uses a socket prosthesis, which is fixed to the soft tissue of the remaining amputation stump via suction or vacuum. The artificial knee joint and/ or lower leg prosthesis can then be attached to the socket. This enables the patients to walk without aids but there are several challenges in the use of a suction prosthesis. One important factor is the length of the remaining stump because it determines the lever arm and the force, which has to be applied for conducting, guiding, and controlling the prosthesis. If the socket does not fit properly it can create skin irritations of the soft tissue, which may lead to sores, ulcers, chronic inflammation with abscesses, and pain.
Moreover, the remaining stump length correlates with the energy expenditure during walking and an amputee uses on average 70% more energy than an able-bodied person. These difficulties can result in a poor gait with negative effects on the remaining musculoskeletal system. This often leads amputees to utilize walking aids or even a wheelchair.
Hence a prosthesis that avoids the skin and soft tissue interface is desirable for different reasons:
– Skin irritation due to friction, chaffing, and squeezing
– An increase in sweating and heat rashes
– Inflammation, bruises and hematoma, pressure marks, and even deep skin injuries
– The dissatisfying fit of the prosthesis due to variation of weight and stump volume
– Pain and missing comfort also during sitting
– Hygienic problems
For a lot of amputees, it is therefore difficult to find their way back into an active lifestyle or to the working force. Often they cannot perform the kind of activity and sports, which they would like to enjoy and they have to rely on the help of others during everyday life. Because of the mentioned difficulties, some single-side or bilateral amputees even depend on a wheelchair permanently.
An osseointegrated, transcutaneous implant creates an alternative to these problems. “Osseointegrated” means “fixed to the bone” and transcutaneous is “perforating the skin”. With this system, the prosthesis is directly attached to the bone and a socket or suction prosthesis becomes unnecessary and dispensable.
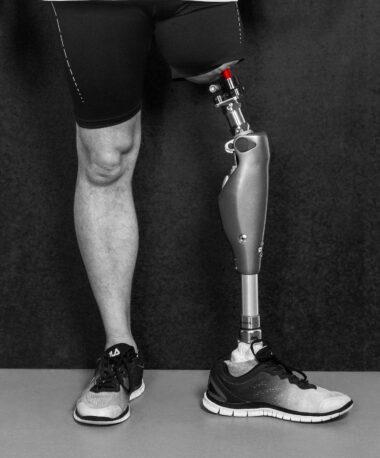

There are no skin irritations due to chaffing, sweat or heat so that the prosthesis can be used for a longer period without causing pain, discomfort, or mobility constraints.
If you would like the best surgeons in Iran’s first-class hospitals to perform your surgery, and at the same time be comfortable and stress-free during your treatment and stay in Iran at a reasonable cost, like your home, get in touch with Iran Medtour Consultants. 😊
Using Endo Exo Prosthetic Implant, people with disabilities can perform activities such as cycling, such as cycling, just like normal people.
Using an Endo-Exo implant, the amputee will be able to walk easily again and can even easily use sports equipment such as a treadmill.

